
Not examining and treating gallstones promptly, refusing surgery to take medicine to dissolve the stones causes many people to have complications with gallstones that are difficult to treat.
In the first 6 months of the year, a medical facility in Ho Chi Minh City received nearly 800 patients with gallstones, of which the rate of complications due to gallstones was three times higher than the same period last year. 38% of these patients suffered from acute cholecystitis.
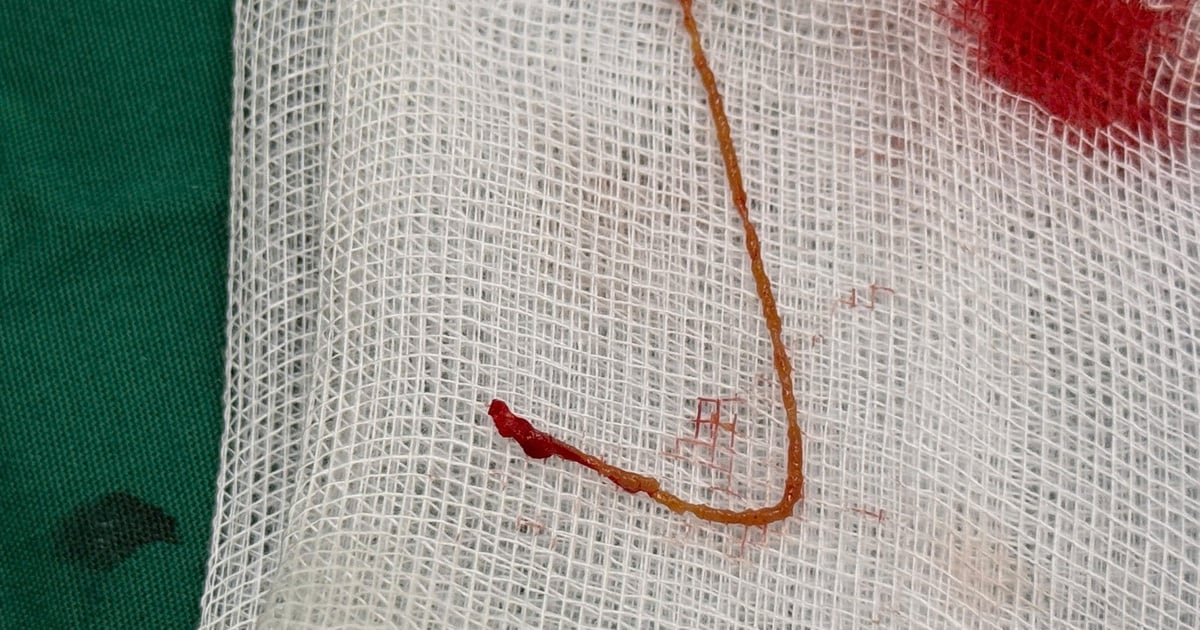
 |
| Illustration photo. |
Doctors explain that the rate of acute cholecystitis is increasing because patients at risk of acute cholecystitis refuse surgery to take gallstone-dissolving drugs, fearing that gallbladder removal will affect their health.
Some people with many diseases such as cardiovascular, respiratory, diabetes, taking antiplatelet drugs, anticoagulants, etc. cannot have surgery. If the patient is not examined by a doctor and advised to have surgery early, the disease will also cause complications if left untreated for a long time.
Gallbladder stones are quite common, tend to progress silently and are difficult to detect early. Patients often come to the doctor late, in many cases even though stones are detected but not treated completely, leading to acute cholecystitis, cholangitis, septic shock, acute pancreatitis, necrotizing pancreatitis...
Like Ms. Hong, 62 years old, Ho Chi Minh City, was admitted to the emergency room due to abdominal pain, fever and chills. A year earlier, she had been treated for necrotizing pancreatitis for about two months at a hospital but was not scheduled to have her gallbladder removed afterwards.
Ms. Hong was not completely treated for necrotizing pancreatitis caused by gallstones before, leading to complications of gallstones falling into the common bile duct, causing bile duct obstruction.
Chronic inflammation of the gallbladder due to gallstones and pancreatitis at the same time causes many adhesions, making it difficult for doctors to determine the structure, and there is a high risk of complications during surgery such as bleeding and bile duct damage.
Typically, these cases undergo endoscopic retrograde cholangiopancreatography (ERCP) to remove common bile duct stones, and laparoscopic cholecystectomy is performed.
However, in Ms. Hong's case, due to the necrotic mass in the head of the pancreas compressing and deforming the duodenum, it was impossible to access and pull out the common bile duct stones through endoscopic cholangiopancreatography. She underwent laparoscopic cholecystectomy and at the same time, the common bile duct was split to remove two stones from the common bile duct.
After surgery, her abdominal pain was gone. A follow-up visit 10 days later showed that the common bile duct was free of stones and her health had recovered well.
Similarly, Mr. Thuan, 64 years old, Ho Chi Minh City was taken to the hospital due to high fever, fatigue, lethargy, and severe abdominal pain in the right hypochondrium and epigastric region (above the navel). Test results showed that the white blood cell count increased to more than 18,000 (normal 4,000-10,000/mm3 of blood).
The doctor diagnosed Mr. Thuan with sepsis due to biliary peritonitis caused by necrotizing cholecystitis - a complication of gallstones. The patient needed emergency laparoscopic cholecystectomy to prevent the disease from worsening.
Dr. Pham Cong Khanh, Head of the Hepatobiliary - Pancreatic Department, Endoscopy and Endoscopic Surgery Center, Tam General Hospital, Ho Chi Minh City, assessed that Mr. Thuan's gallbladder was necrotic, so the surgery could have complications such as bleeding and bile duct damage.
Patients with a history of cerebral infarction, high blood pressure, atrial fibrillation with rapid ventricular response, and type 2 diabetes are at high risk of respiratory failure and cerebrovascular accident during and after surgery.
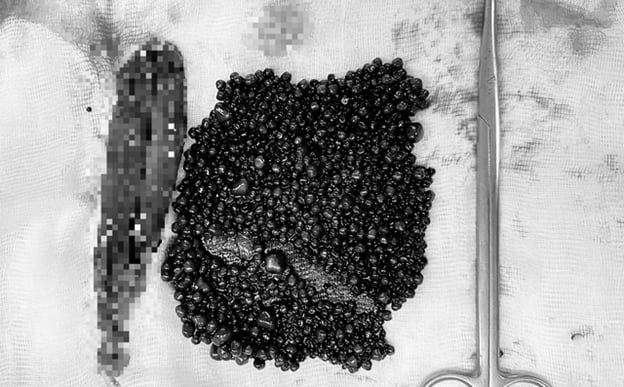
During the surgery, the doctor noted cloudy fluid and a small amount of pseudomembrane around the gallbladder, necrosis of the gallbladder wall at the base, and after cutting the gallbladder, two stones measuring 0.5 cm were removed. One day after the surgery, Mr. Thuan no longer had symptoms of abdominal pain or fever and was discharged after 5 days.
Indications for surgery: Painful stones of any size (under 0.6 cm have a high risk of causing obstruction of the cystic duct leading to acute cholecystitis, pancreatitis due to falling into the main bile duct). Stones over 2 cm, over time, increase the risk of complications such as compression of the main bile duct causing biliary obstruction.
Early stage stones are often treated with medication, when stones show symptoms, gallbladder surgery is required.
The most common treatment is laparoscopic cholecystectomy. Indications for cholecystectomy are an art so that patients do not have their gallbladders removed for no reason due to diseases with similar symptoms, nor do they take ineffective gallstone-dissolving drugs until the disease becomes severe.
Gallstones are easily detected by abdominal ultrasound with high accuracy. Patients need to proactively have regular health check-ups. People with symptoms of cholecystitis such as right lower quadrant pain, high fever, chills, etc. should see a doctor immediately.
Source: https://baodautu.vn/lien-tiep-benh-nhan-nhap-vien-do-bien-chung-soi-mat-d220797.html

![[Photo] National Assembly Chairman Tran Thanh Man attends the Policy Forum on Science, Technology, Innovation and Digital Transformation](https://vstatic.vietnam.vn/vietnam/resource/IMAGE/2025/4/13/c0aec4d2b3ee45adb4c2a769796be1fd)


![[Photo] Prime Minister Pham Minh Chinh chairs the Government's special meeting on law-making in April](https://vstatic.vietnam.vn/vietnam/resource/IMAGE/2025/4/13/8b2071d47adc4c22ac3a9534d12ddc17)









![[Photo] Free health check-up for policy families in Cu Chi district](https://vstatic.vietnam.vn/vietnam/resource/IMAGE/2025/4/13/d2abdd768f84432aac3cc82cb6b58fa8)


























































![[Podcast]. Kites and Childhood](https://vstatic.vietnam.vn/vietnam/resource/IMAGE/2025/4/13/a4697c2294a843f39084a21134c3feb0)











Comment (0)