
Diphtheria can occur at any age, but 70% occur in children under 15 years of age who have not been vaccinated. Myocarditis is one of the particularly serious complications of diphtheria.
Diphtheritic myocarditis occurs in 10%–20% of cases of respiratory diphtheria.
Diphtheria is an acute, epidemic infectious disease, mainly transmitted through the respiratory tract, caused by diphtheria bacilli (Corynebacterium diphtheriae).
The source of diphtheria is infected patients or healthy people who carry the bacteria but do not show symptoms of the disease. The disease is mainly transmitted through the respiratory tract when in contact with droplets of infected people when coughing or sneezing. In addition, the disease can be transmitted indirectly when in contact with objects contaminated with nasal secretions from infected people. The disease can also be transmitted when in contact with skin areas damaged by diphtheria.

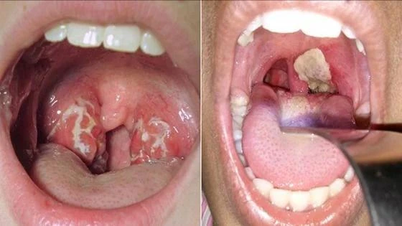
Clinical symptoms usually begin 2-5 days after nasopharyngeal infection and may include sore throat, malaise, cough, hoarseness, painful swallowing, bloody nasal discharge, and salivation. Fever is usually mild or absent. The lesions are characterized by a grayish-white membrane that initially covers the tonsils and then rapidly spreads to the uvula, soft palate, and posterior pharyngeal wall.
In severe cases, the damage causes airway obstruction, respiratory failure. Systemic damage occurs when diphtheria toxin spreads into the bloodstream, leading to toxin-mediated damage to the heart, kidneys, and peripheral nerves.
Doctor Hoang Cong Minh, National Heart Institute, Bach Mai Hospital said that diphtheria exotoxin secreted affects the heart, causing arrhythmia and can lead to sudden death due to heart failure. Myocarditis complications often occur when the patient is in the acute stage or a few weeks after recovery. In cases where myocarditis appears in the early days of the disease, the patient has a poor prognosis and a high mortality rate.
Cardiac complications are common and well documented in diphtheria because of the high affinity of diphtheria toxin for myocardial cells and the cardiac conduction system. Myocarditis occurs due to degeneration of actin myofibers caused by diphtheria toxin, leading to impaired myocardial contractility. In patients who recover from the disease, damaged myocardial cells are replaced by fibrotic tissue, which may leave long-term cardiac sequelae.
Cardiovascular manifestations in diphtheria are very diverse but the most typical are myocardial contractility dysfunction and arrhythmia, sometimes with pericarditis and endocarditis.
Diphtheritic myocarditis occurs in 10%–20% of cases of respiratory diphtheria, although the actual number may be higher. Notably, this complication occurs almost exclusively in unvaccinated or incompletely vaccinated individuals.
Myocarditis usually presents late in the second week but may present earlier in severe infections. Diphtheritic myocarditis has a case fatality rate of 60%–70%.
Today, modern monitoring and diagnostic methods, such as invasive blood pressure monitoring, continuous electrocardiographic monitoring, and echocardiography, can help diagnose and manage and detect cardiac dysfunction and arrhythmias early.
Treatment of myocarditis
Diphtheritic myocarditis is currently mainly treated with supportive measures to maintain normal hemodynamic parameters. Antiarrhythmic drugs are usually only used for rapid and sustained arrhythmias.
Dr. Minh said that prophylactic treatment of arrhythmias is not recommended. Temporary pacemaker placement may be used in patients with severe diphtheria-induced myocarditis and bradyarrhythmias. The success of temporary pacing depends on the extent of conduction system damage and myocardial reserve.
Treatment of diphtheria includes early administration of diphtheria antitoxin and antibiotics. Daily mortality increases with delay in diphtheria antitoxin administration, from 4.2% in the first two days to 24% by the fifth day of illness.
Antitoxin is considered the cornerstone in preventing severe complications and must be readily available. In Vietnam, only a few tertiary hospitals have diphtheria antitoxin available for early treatment.
"Myocarditis is the most serious complication of diphtheria and the most common cause of death. Although this is considered a life-threatening condition, if anti-diphtheria serum is used promptly and intensive supportive care is provided, the disease can be successfully treated," Dr. Hoang Cong Minh emphasized.
Source
![[Photo] General Secretary To Lam receives the Director of the Academy of Public Administration and National Economy under the President of the Russian Federation](/_next/image?url=https%3A%2F%2Fvphoto.vietnam.vn%2Fthumb%2F1200x675%2Fvietnam%2Fresource%2FIMAGE%2F2025%2F12%2F08%2F1765200203892_a1-bnd-0933-4198-jpg.webp&w=3840&q=75)








































































































Comment (0)